

Основные моменты
- DGL — это форма солодки, которую люди изменили для более безопасного потребления.
- Женщины традиционно использовали корень солодки, чтобы сбалансировать свои гормоны во время менструации и менопаузы.
- Необходимо провести дополнительные исследования, чтобы определить, эффективна ли солодка для лечения кислотного рефлюкса.
Доступны многие методы лечения кислотным рефлюксом. Большинство врачей рекомендуют безрецептурные (внебиржевые) лекарства. Альтернативные методы лечения также могут облегчить ваши симптомы. Одним из таких вариантов является деглицирризиновая солодка (DGL). Люди считают, что использование этого несколько раз в день будет облегчать симптомы кислотного рефлюкса.
Кислотный рефлюкс возникает, когда нижний сфинктер пищевода (LES) полностью не закрывается. ЛЕС печатает пищу и кислоту, которая ломает пищу, в желудке. Если ЛЕС полностью не закрывается, кислота может перемещаться вверх по пищеводу. Это может вызвать жжение.
DGL — это форма солодки, которую люди обрабатывали для более безопасного потребления. Они удаляют значительное количество вещества, называемого глицирризином. Это делает DGL пригодным для длительного использования. Большинство солодки происходит из Азии, Турции и Греции. Вы можете найти DGL в нескольких формах, чаще всего в таблетках или капсулах.
Feature Summary
Deglycyrrhizinated licorice, or DGL, has been used clinically for decades, primarily for the treatment of peptic ulcers.1 Licorice has many triterpenoids and hundreds of flavonoids that have been shown to inhibit several inflammatory enzymes, including both cyclooxygenase-2 (COX-2) and 5-lipoxygenase (5-LOX). These enzymes decrease the production of several potent inflammatory compounds, including IL-6, prostaglandin E2, thromboxane B2, and leukotriene B4.2 Importantly, this inhibition is not primarily due to glycyrrhizic acid, the component of licorice that has been removed in DGL and that is associated with mineralocorticoid excess and hypertension.3 Licorice has multiple active compounds with anti-inflammatory, anti-microbial, and anti-allergic actions, including glabridin and at least seven licochalcones. The compounds have been shown to prevent lipopolysaccharide (LPS) induced production of inflammatory compounds, inhibit yeast and bacterial biofilm formation, and upregulate antioxidant enzymes.4-6
Clinically, DGL has been shown to have comparable efficacy to cimetidine for both the healing and prevention of ulcer recurrences.7 Additionally, extracts of licorice have been shown to inhibit the adhesion of H. pylori to gastric mucosa, as well as the growth of antibiotic resistant strains, suggesting multiple mechanisms of action for its anti-ulcer benefit.8,9 The use of chewable tablets appears necessary for DGL’s efficacy as it allows for distribution and absorption by the gastric mucosa.
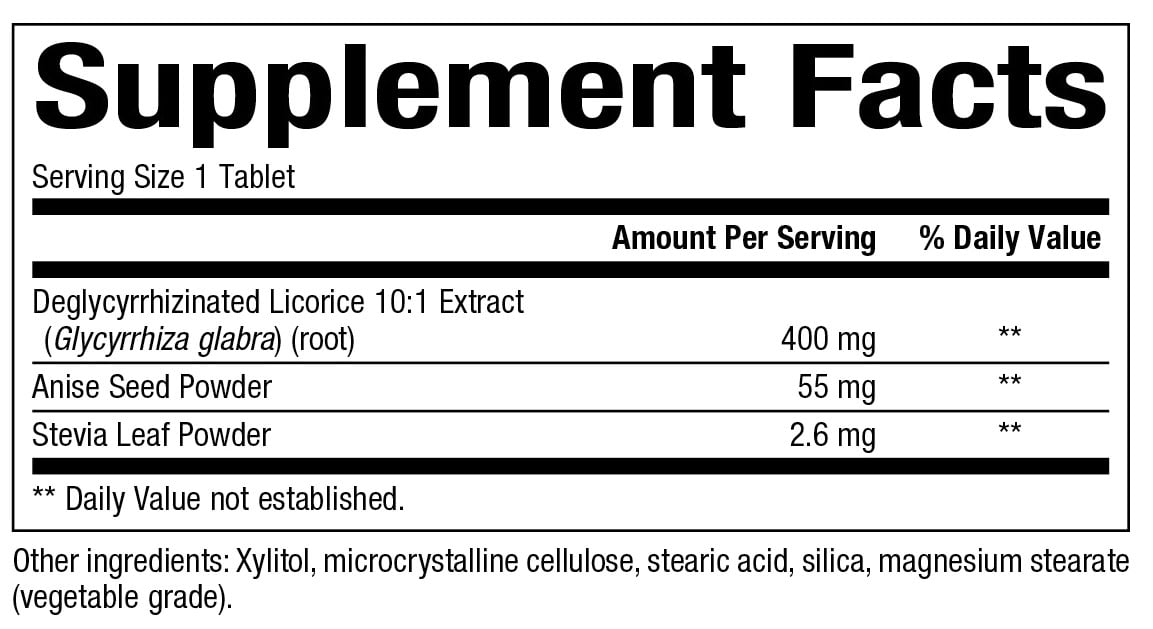
Supplement Facts:
Dosage:
Suggested Usage: Chew 1 tablet 20 minutes before each meal or as directed by a health care professional. Consult a health care professional for use beyond 16 weeks.
Allergens:
Contains no artificial colors, preservatives, or sweeteners; no dairy, starch, sugar, wheat, gluten, yeast, soy, egg, fish, shellfish, animal products, salt, tree nuts, or GMOs. Suitable for vegetarians/vegans.
Drug Interactions
No known drug interactions. Licorice influences the activity of several cytochrome enzymes and reduces warfarin activity in animal models, likely due to glycyrrhizic acid activity. DGL use should be carefully monitored in these patients.
1. Turpie, A G., Runcie, J., Thomson, T.J. (1969). Clinical trial of deglydyrrhizinized liquorice in gastric ulcer. Gut, 10(4), 299-302.
2. Yang, R., Wang, L.Q., Yuan, B.C., et al. (2015). The pharmacological activities of licorice. Planta Med, 81(18), 1654-69.
3. Chandrasekaran, C.V., Deepak, H.B., Thiyagarajan, P., et al. (2011). Dual inhibitory effect of Glycyrrhiza glabra (GutGard™) on COX and LOX products. Phytomedicine, 18(4), 278-84.
4. Yehuda, I., Madar, Z., Szuchman-Sapir, A., et al. (2011). Glabridin, a phytoestrogen from licorice root, up-regulates manganese superoxide dismutase, catalase and paraoxonase 2 under glucose stress. Phytother Res, 25(5), 659-67.
5. Maria Pia, G.D., Sara, F., Mario, F., et al. (2019). Biological effects of licochalcones. Mini Rev Med Chem, 19(8), 647-56.
6. Ahn, S.J., Cho, E.J., Kim, H.J., et al. (2012). The antimicrobial effects of deglycyrrhizinated licorice root extract on Streptococcus mutans UA159 in both planktonic and biofilm cultures. Anaerobe, 18(6), 590-6.
7. Maria Pia, G.D., Sara, F., Mario, F., et al. (2019). Biological effects of licochalcones. Mini Rev Med Chem, 19(8), 647-56.
Licorice root has been widely used as herbal medicine dating back to at least 500 BC.1 Traditional applications across diverse cultures include as both a demulcent and an antiinflammatory, often used to soothe respiratory or gastrointestinal (GI) symptoms. Modern botanical applications of the herb continue this tradition, with recommendations including the treatment of gastric ulcers, bronchitis, cough, and dyspepsia.2 While licorice is indispensable in these and many other herbal applications, it comes with a slight but measurable risk of side effects when used as a whole-root extract.
One of the constituents in licorice root is glycyrrhizin, a triterpene glycoside that has been shown to have aldosterone-like effects.3 High doses or chronic consumption of glycyrrhizin from licorice root can create side effects that mimic a hypermineralcorticoid state. Clinically, this presents as electrolyte imbalances, hypertension, and possible cardiac abnormalities. While side effects are not common and risk is further minimized with monitoring of the patient and knowledge of proper dosing, removal of the glycyrrhizin compound eliminates the risk altogether. Today, deglycyrrhizinated licorice (DGL), which is specifically marketed for GI complaints, is a popular over-the-counter supplement.
While DGL is popular for relieving gastric irritations, clinical trial support is weak. DGL exemplifies a widely accepted natural agent that “works” when assessed empirically but has yet to meet criteria for inclusion in an evidence-based, conventional medical paradigm.
Modern History
Support for the Beneficial Effects of DGL
Much of the in vitro data on licorice root is on glycyrrhizin, with less information available on the other constituents of licorice. For example, glycyrrhizin and its derivatives have been shown to effectively kill Helicobacter pylori strains, including those that are clarithromycin-resistant or metronidazole-resistant.8 Various flavonoids found in DGL have also been shown to be bactericidal toward H pylori and may account for some of the antiulcer activity preserved with the removal of glycyrrhizin.9 In addition, DGL has demonstrated the ability to increase mucin, possibly by increasing the number of mucous secreting cells in the stomach.10
Deglycyrrhizinated licorice exemplifies a widely accepted natural agent that “works” when assessed empirically but has yet to meet criteria for inclusion in an evidence-based, conventional medical paradigm.
Clinical Evidence to Date
Four different licorice medicaments are used in clinical studies on ulcerative diseases, and differentiation among them is essential to an accurate review of the literature. The 4 include crude extracts of the whole plant, DGL combined with other agents (ie, Caved-S), DGL alone, and drug analogs of glycyrrhizin derivatives (eg, carbenoxolone, enoxolone). Many reviews, references, and marketing materials on DGL report on these 4 forms interchangeably. A closer look at this indiscriminate use of clinical trial data shows that they are not equivalents, and extrapolation of studies using agents containing glycyrrhizin or glycyrrhizin-like compounds are not relevant when compiling trial data on DGL.
Crude extracts of licorice are a traditional use of the plant and led to the initial interest of Revers and others in proving its therapeutic use for ulcers. Since the crude extract contains glycyrrhizin, and glycyrrhizin has been shown to heal ulcerative lesions as a single agent, the efficacy of licorice crude extract can be assumed to be at least partly due to the glycyrrhizin content. DGL by definition is lacking glycyrrhizin; therefore its efficacy in ulcerative complaints must be proven independently from data on crude extracts.
Carbenoxolone (Biogastrone™), a synthetic analogue of the biologically active metabolite of glycyrrhizin, β-glycyrrhetinic acid, is an approved drug in the United Kingdom and Europe for ulcers and aphthous stomatitis. Carbenoxolone and the newer analogue, enoxolone, both have a well-documented risk of inducing symptoms of a hypermineralcorticoid state. The induction of side effects with a glycyrrhetinic acid analogue is to be expected, as glycyrrhizin and its metabolites have long been identified as the agents inducing these side effects.5 As synthetic analogues of the very constituent that was removed from DGL, there should be no extrapolation of clinical trial data derived from carbenoxolone or enoxolone as support or repudiation of DGL’s efficacy in ulcerative complaints.
A comparison of the results derived from these trials provides conflicting results without trend or obvious conclusions able to be drawn. A cursory look at the summary of clinical trials (Table) shows no standard dosage, delivery, trial duration, or methodology used in the majority of trials. How efficacy was assessed varied between the trials as well with questionnaires, clinical observation, barium radiography, or endoscopic assessments used.
In another trial by W. Larkworthy and colleagues, the intervention closely matched the above intervention of over 4 g daily, except it used DGL as a single agent and there was a mastication group to see if chewing conferred any benefit.13 This trial, which assessed patients endoscopically, did not show statistical difference in the healing of ulcers between the intervention and placebo groups. This may be due to the suggestion of 5 meals per day for all study participants. This frequency of eating increased the salivation of all participants, which has been independently proven to have an antiulcer effect.14 Further trials assessing the efficacy of these high doses are warranted to definitively answer the question of statistically significant effects of DGL.
As an aside, Larkworthy and colleagues suggest that further trials must include endoscopic assessment, as symptoms do not always correlate with healing of ulcers. This suggests that licorice’s pain-relieving abilities should be assessed separately from its ability to visibly increase the rate of healing in future trials.
Abbreviations: DGL, deglycyrrhizinated licorice; RCT, randomized controlled trial.
Conclusion
DGL для кислотного рефлюкса

В чем преимущества DGL?
- DGL может увеличить производство слизи. Это может защитить желудок и пищевод от кислоты.
- Ранние данные свидетельствуют о том, что экстракт солодки может помочь лечить гепатит С.
- Солодка может лечить язвы.
Традиционно женщины использовали корень солодки, чтобы сбалансировать свои гормоны во время менструации и менопаузы. Сегодня солодка присутствует в некоторых домашних средствах.
Люди считают, что солодка облегчает боль в горле, лечит язвы и помогает очищать респираторные инфекции, такие как бронхит.
Корень солодки может даже лечить вирусные инфекции, такие как гепатит. Клинические испытания показали, что инъекционная форма экстракт солодки имеет эффекты против гепатита С, которые являются полезными. Необходимо провести дополнительные исследования, чтобы определить, является ли это приемлемым вариантом лечения.
Некоторые врачи и альтернативные защитники здоровья рекомендуют DGL для кислотного рефлюкса. Люди полагают, что DGL способствует активности слизи. Эта дополнительная слизь может выступать в качестве барьера для кислоты в желудке и пищеводе. Этот барьер может позволить поврежденной ткани заживать и предотвращать появление кислотного рефлюкса в будущем.
В настоящее время научные исследования по использованию солодки не нашли достаточных достоверных данных для определения того, эффективна ли лакрица для лечения любого состояния.
Риски и предупреждения
Администрация США по контролю за продуктами и лекарствами не регулирует травяные добавки и другие альтернативные методы лечения.В зависимости от производителя ингредиенты добавки могут различаться.
Вам не следует использовать лакричник, если вы принимаете диуретики, кортикостероиды или другие лекарства, которые снижают уровень калия в вашем организме. Солодка может усилить эффекты этих препаратов и привести к тому, что уровень калия станет опасно низким.
Люди, у которых сердечная недостаточность или высокое кровяное давление, должны проявлять осторожность при приеме лакричника. Женщины, которые беременны, должны избегать использования солодки в качестве дополнения, поскольку это может увеличить риск преждевременных родов.
Во всех случаях лечения кислотного рефлюкса лучше поговорить с врачом. Если вы используете альтернативную терапию, которую не назначал ваш врач, вы должны сообщить им об этом. Это поможет им определить лучший уход и избежать возможных конфликтов с другими методами лечения.
Другие виды лечения
Другие варианты лечения рефлюксной рефлюкс
Многие лекарства на рынке могут облегчить симптомы рефлюкса кислоты, а также лечить состояние.
Антациды могут нейтрализовать кислоту желудка и обеспечить временный рельеф для кислотного рефлюкса. Вы должны взять их только на короткий период. Они лучше всего подходят для людей с редким кислотным рефлюксом.
Блокаторы H2 и ингибиторы протонного насоса (PPI) контролируют желудочную кислоту в течение более длительного периода времени, чем антациды. Некоторые из них доступны через стойку. Это включает фамотидин (Пепсид) и омепразол (Прилосец). Ваш врач может также назначить более сильные версии этих препаратов, если это необходимо.
У каждой формы лекарства есть побочные эффекты. Антациды могут вызывать диарею и запор. Блокаторы H2 и ИЦП могут увеличить риск перелома костей или дефицита B-12. Вы должны проконсультироваться с врачом, если вы принимаете какое-либо лекарственное средство с рефлюксным кислотным рефлексом в течение более двух недель.
В редких случаях вам может потребоваться операция по восстановлению нижнего сфинктера пищевода.
Еда на вынос
Вынос
Кислотный рефлюкс — общее заболевание, которое может вызвать серьезный дискомфорт и повредить ваш пищевод. Примерно 1 человек из 10 человек переживает это каждую неделю. Около 1 человека из 3 симптомов испытывает каждый месяц.
Вы должны работать со своим врачом, чтобы определить лучший план лечения для вас. Если вы решите попробовать альтернативную терапию, такую как DGL, вы должны сообщить своему врачу. Они могут поговорить с вами о любых побочных эффектах и убедиться, что это не повлияет на какие-либо лекарства, которые вы сейчас принимаете. Читайте дальше для других альтернативных методов лечения кислотного рефлюкса.
")




")