

 A root canal is the pulp-filled cavity in the root of a tooth, containing both nerves and blood vessels. When this area of the tooth becomes infected or inflamed, endodontic therapy may be needed. Performed by a dentist or endodontist, root canal therapy removes the infected tissue in an effort to prevent the infection from spreading and save the natural tooth.
A root canal is the pulp-filled cavity in the root of a tooth, containing both nerves and blood vessels. When this area of the tooth becomes infected or inflamed, endodontic therapy may be needed. Performed by a dentist or endodontist, root canal therapy removes the infected tissue in an effort to prevent the infection from spreading and save the natural tooth.
Root canal –
When These Two words comes in
mind that that strike fear of pain and everybody want to know the answer of
this hell question of pain, “What is root canal treatment?”
Most people feel pain when they hear the words “root canal”, but done correctly, a root canal actually relieves pain. But, this is the right query, what is a root canal? Who needs one and why? What is the process and what can you expect if you are getting one?
Book Now:Advanced Full Body Check Nearby you at 50% OFF, NOW (Lowest Price)
What is a Root Canal?

Root canal is a dental treatment
to repair a badly damaged tooth instead of removing it. The term “root
canal” means cleaning of the canals inside a teeth’s root. It is a dental
procedure that cleans the tooth from inside when the pulp in the tooth has
become infected.
This could happen due to:
- A Tooth Abscess
- Severe tooth decay
- Facial/mouth/tooth trauma
- Needing a crown
- Cracked tooth or filling
Generally a patient will feel the
tooth pain, sensitivity, soreness & swelling, and discoloration in infected
tooth. If you’re facing these symptoms – meet your dentist, as this pain may be
you need a root canal treatment!
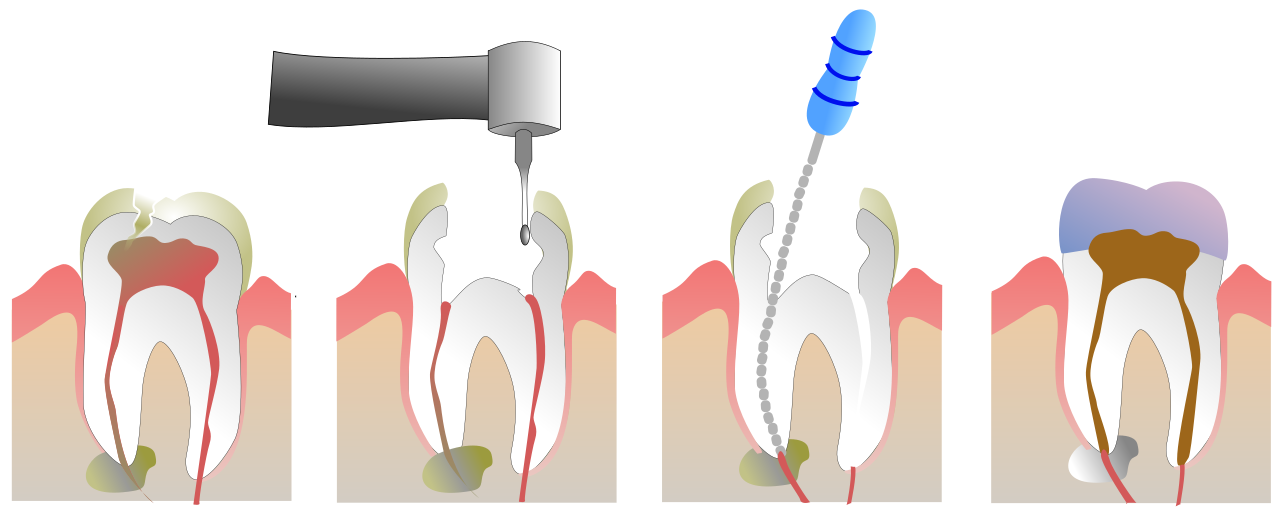
Treatment Steps to a Root Canal:

- Firstly, an x-ray is needed to check the extent
of infection and to see the entire tooth area. - Local anesthesia is applied to keep the patient
comfortable from pain during the treatment procedure. - Rubber sheeting is placed around the tooth to
keep it dry. A rubber guard keeps saliva away from the tooth that is being
worked on to ensure safety. - The dentist creates an opening in the tooth that
allows them to clean the inside the tooth. - After cleaning and shaping the inside the tooth,
a special type of filling has to be done. Filling the space where the tooth
pulp was removed that helps to prevent reinfection and also helps strengthen
the tooth. - A crown is used to complete the restoration.
What is Root Canal Treatment?
ALSO Read: Dental Home Remedies To Get Rid Of Yellow Teeth
Root Canal Treatment is the entire procedure of diagnosing, and dental care treatment to reduce your tooth pain and improve your dental health.
The primary goal of root canal
therapy is to save the tooth, which means you can get back to enjoying the food
you love without pain. The whole procedure includes a few dentist meetings, and
with new advanced technology made this faster & more effective than ever
before.
The prospect of undergoing a root canal is enough to flood many people with fear. Though we’ve learned to dread the very phrase, root canals are often highly successful dental procedures that are not any more uncomfortable than having a cavity filled.
Here’s what to know about root canals, how the procedure works and who may need one.
A root canal, or endodontic therapy is a standard dental procedure used to remedy an infection caused by a cavity or injury to the tooth. It can be performed by a general dentist or endodontist, and save your tooth from extraction by removing infected nerve tissue and bacteria from inside your tooth.
Who Needs a Root Canal?
You’ll likely need a root canal when the inner layer of your tooth has deep decay.
“A tooth is essentially composed of three parts: enamel, dentin and then the pulp,” says Alex Rubinov, D.D.S., Ph.D., a practicing dentist in New York City. “The pulp has a canal which allows the tooth to communicate with the body by way of fibers and blood vessels.” A root canal is needed when the pulp is impacted by trauma or deep tooth decay, he explains.
While an X-ray will indicate if the pulp is infected and a root canal is necessary, common symptoms include:
- Sensitivity to hot or cold food or drinks
- Pain when chewing
- Loose tooth
- Swollen gums, cheek or jaw
- Tooth discoloration
- Discharge from tooth
“The infection may also be painless if the inflammation and purulence can drain into your sinus, or through the gums,” adds Dr. Loetscher. “In this case, you may be unaware of it.” This could lead to sinusitis, or a sinus infection.
“When an infection drains through the sinus or gums, it spreads slower because the infection is not accumulating in the bone or gums, neck and what is called soft tissue. These teeth that have ‘drainage’ tend to be the most asymptomatic, and slowest to cause problems,” expplains Dr. Loetscher.
How Does the Root Canal Procedure Work?
A root canal may be completed in one or more appointments depending on the severity of the infection, according to Ghaznia Khan, D.D.S., a general dentist in Fort Worth, Texas.
What to Expect During a Root Canal
- Your dentist gives you a local anesthesia, such as Novocaine, to make you comfortable during the treatment.
- A small opening is drilled in your tooth, says Dr. Loetscher. For back teeth, this happens on the top of the tooth. For front teeth, the hole is made in the back.
- Your dentist then removes the infected pulp and cleans the canals, adds Dr. Rubinov. Medicine is then applied to the canals and remains on the tooth until your next visit.
- The canals are sealed and your dentist fills the pulp chamber with a material called gutta percha.
What to Expect After a Root Canal
While patients may feel a pinch when a needle pokes the gum around the affected tooth to numb it, “the actual root canal procedure is not painful,” adds Dr. Rubinov. “The reason pain is associated is most commonly due to the sensitivity leading up to the procedure. A neglected infection can lead to swelling or an abscess, which is what causes the pain.”
If the root canal was performed on a back tooth, you will require a crown, or tooth-like cap that supports a tooth after it has been weakened, explains Dr. Loetscher. “If you fail to have the tooth crowned it will split one day, requiring extraction.”
How Much Does a Root Canal Cost?
- Front Tooth: $620 to $1,100
- Premolar: $720 to $$1,300
- Molar: $890 to $1,500
Most insurance plans cover between 50% to 80% of the cost if you’ve already met your deductible.
The type of dental office you visit may affect the cost, too. Seeking treatment under a general dentist may be more cost-effective than seeing an endodontist, says Dr. Loetscher. But he notes complicated procedures like those performed on molars are often referred to an endodontist.
What Happens If You Skip a Root Canal?
Declining a root canal procedure is not advisable, as you will need to address the infection in your tooth. Ignoring the issue, Dr. Khan says, often results in one of these scenarios:
- An abscess or infection spreading to other areas such as the jaw bone or sinuses
- Tooth loss
“Eventually the infection will worsen, likely having pain, bone loss and not a healthy situation,” adds Dr. Loetscher. “This typically occurs over the course of a few weeks.”
If you’re feeling nervous over an impending root canal, there are plenty of options to help make you more comfortable. For his patients, Dr. Rubinov leans on medications, like nitrous oxide to help ease anxiety, and things like noise-canceling headphones, eye masks and stress balls.
Your Smile, For Life
You own your smile, and you should own it forever. With Byte, watch your smile transform with digital access to your doctor-directed treatment plan.
$80 Off With Code FORBESBBP
Canberra, ACT, Australia
The majority of endodontic failures can often be attributed to the inability of localising and treating all the canals of the root canal system. Root canal systems are commonly complex with the teeth often having lateral ramifications, extra roots or additional canals. Molar and premolar teeth can present with the highest incidence of aberrant morphology. A thorough knowledge of expected anatomy and variations from the norm are essential when undertaking root canal therapy to ensure success.
The clinical impact of missed anatomy may result in failure and the necessity to carry out costly root canal re-treatment. Prevention of missed anatomy begins with a thorough knowledge of common tooth morphology. The clinician must be aware of the complexities of the root canal system and anatomical variations of the norm that may be encountered according to tooth type. The human dental pulp manifests multiple configurations and shapes which can vary from one individual to another. Careful interpretation of preoperative angled radiographs, correct access extension and a detailed exploration of the interior of the tooth using magnification and illumination are key steps for achieving clinical and radiographic success.
Overview of Root Canal Anatomy
Schematic diagrams representing Weine’s classification of root canal configurations. – single canal from pulp chamber to apex. – two canals leaving the chamber and merging to form a single canal short of the apex. – two separate and distinct canals from chamber to apex. – one canal leaving the chamber and dividing into two separate and distinct canals
Vertucci classification. a single canal with one foramen. two canals that join in the apical third. – one canal that divides into two that subsequently reunites and exits as one. – two separate canals all the way to the apex. one canal that divides just short of the apex. two canals that unite in the root and divide again at the apex. one canal that divides, reunites and finally exits through two apical foramina. three separate canals in one root
Maxillary Central Incisor Teeth
The root of the maxillary central incisor is often bulkier than the lateral with cross-sectional anatomy varying from triangular, circular or oval in shape. The canal is often tapering towards the apex in mature teeth with minimal curvatures in the apical portion (Fig. ).
Overview of maxillary permanent central incisor teeth
The access cavity is initiated by penetrating the bur occlusal to the cingulum, avoiding the incisal edge. Once penetration to the root canal is achieved, the access cavity must be refined in a mesio-distal direction to remove the entire roof associated with the pulp horns. The access cavity achieves a roughly triangular shape with this preparation, which mirrors the anatomy of the pulp chamber (see Fig. ).
Clinical photographs showing step-by-step access preparation in an anterior maxillary central incisor. Note () preoperative view ( representing intended triangular access incorporating pulp horns), () initial bur penetration, () root canal penetrated, () widening of access in a mesial and distal direction to ensure pulp horns are incorporated, () use of ultrasonics to remove overhanging dentine and to ensure pulp horns are free of any tissue remnants and () final access preparation completed
Maxillary Lateral Incisor Teeth
The lateral incisor is often smaller in comparison to its neighbouring central counterpart. The root is often slender with an apical curvature generally in a disto-palatal direction.
The presence of extra roots or occurrence of developmental grooves is more likely in this tooth group. Tooth invaginations (dens in dente) are also a common finding, which complicates endodontic management. Early recognition is essential and referral is probably best considered (Fig. ).
Overview of maxillary permanent lateral incisor teeth
In this tooth, the access cavity is created in the same way as in the central incisor. The pulp horns are often closely situated or singular in this tooth, resulting in a final shape that is more likely to be ovoid as opposed to triangular. Care must be taken when negotiating the apical curvature in this tooth, particularly with larger file sizes, which can result in canal transportation or ledging if not correctly identified (see Fig. ).
Maxillary Canine Teeth
These teeth can be one of the longest encountered with roots that are irregularly tapered and wide in a labio-palatal direction. The canal is typically a type I configuration with a root curvature apically often in a distal direction although can occur in any direction (Fig. ).
Overview of maxillary permanent canine teeth
The access cavity begins about halfway up the crown on the palatal side (see Fig. ). With an ovoid pulp chamber and a single horn, the access cavity is oval in outline and shape. The root canal is quite straight in the coronal and middle third and long enough to require the use of long 30-mm instruments.
Clinical photographs demonstrating access cavity preparation in a maxillary canine tooth. Note () preoperative view and () completed access preparation showing ovoid outline
Canines with a normal crown and root but with two canals are rare and difficult to identify because the canals may be superimposed. An adequate pulp chamber opening and careful observation of intra-operative radiographs may help in these difficult cases.
Maxillary Premolar Teeth
The maxillary first premolar has variable morphology but is generally considered to have two roots and two canals (see Fig. ). The second premolar although variable at times generally presents with a single-rooted single canal system (see Fig. ).
Overview of maxillary permanent first premolar teeth
Overview of maxillary permanent second premolar teeth
Careful radiographic assessment is essential in order to ascertain the likely number of roots and canal morphology before any operative intervention. Peri-apical radiographs give a two-dimensional image of a three-dimensional root canal system, so a minimum of two radiographs should be taken to reveal external and internal features of the tooth. A parallel radiograph should be taken with either a mesial or distal horizontal tube shift. The second angled radiograph may help visualise superimposed roots, displace the zygomatic process of the maxillary bone and increase the chances of observing additional root canals present.
The intra-oral radiograph should be carefully inspected for any sudden changes in the radiographic density of the root canal space, which may indicate bifurcation or trifurcation of the roots. Any sudden narrowing or disappearance may indicate branching of the root canal system often encountered in these teeth. The same principles can be applied during peri-operative treatment whereby any asymmetry of the file placed in the canal can also indicate the presence of a second root system.
The pulp chamber of the upper first and second premolar is oriented more towards the bucco-lingual direction since in the great majority of cases, it has two canals beneath the respective cusps (see Figs. and ). The point of entry of the bur is the middle of the central sulcus drilling parallel to the long axis of the tooth.
Preoperative clinical photograph showing () occlusal anatomy of an upper maxillary premolar tooth and () completed ovoid access preparation extended in a bucco-palatal direction
Clinical radiographs and photographs demonstrating endodontic treatment of a maxillary first premolar tooth with two canals. Note () preoperative radiograph demonstrating a two-rooted tooth, () MAF, () cone fit and () final obturation showing Vertucci IV canal configuration
The floor of the pulp chamber should be carefully examined looking at the position and symmetry of the canals. Asymmetry is often a good indication of additional anatomy that may be present. Upper premolars with three canals require a modified access cavity with a mesio-distal extension in the buccal portion of the traditional cavity. This modification, resulting in a T-shaped access, permits good access to both buccal canals. The presence of three canals is higher in the first premolar compared to the second but nevertheless rare. The anatomical roots are similar to the first molar whereby an MB, a DB and a P root may be present.
Treatment of maxillary premolars requires extra attention due to their extreme variability that can be encountered. Caution is advised due to the higher risk of failing to treat all internal anatomy, and a dental operating microscope or other forms of magnification are a necessary tool when dealing with these teeth.
Maxillary Molar Teeth
The literature shows a wide variation in anatomy of the maxillary molars although the average tooth often has three roots and four canals (see Figs. and ). The palatal root is often the longest with a curvature in the apical third towards the buccal. The disto-buccal root, which is shorter in comparison, may curve towards the mesial or distal in the apical third. The mesio-buccal root shows the greatest variation with a root that is broad in the bucco-palatal plane and narrowing in the mesio-distal place. This ribbon-shaped root will generally exit the crown mesially but can commonly abruptly curve towards the distal. Curvatures are often encountered in the apical third with possibilities of convergence and joining of additional mesio-palatal canals if present (see Fig. ).
Overview of maxillary permanent first molar teeth
Clinical photographs demonstrating cleared maxillary first permanent molar teeth showing complex canal anatomy. () Maxillary first permanent molar showing the MB root. Note Vertucci classification VI (2–1–2) with a lateral canal from the MB1 canal. () Maxillary first permanent molar with two palatal canals. Note Vertucci classification II (2–1) with interconnecting fins and communication between both canals
Access preparation will be mesial to the external oblique ridge, allowing it to be maintained during preparation whereby enhancing the structural strength of the tooth. The orifice of the palatal canal is often the most prominent beneath the mesio-palatal cusp. The mesio-buccal canal often lies directly beneath the mesio-buccal cusp tip and the disto-buccal canal can often be found 2–3 mm distal to this canal and slightly towards the palatal. Careful inspection of the floor of the pulp chamber may reveal additional anatomy.
Recommended clinical approaches when treating maxillary molars include:
Take two diagnostic radiographs, one parallel and one either with a mesial or distal tube horizontal tube shift, to correctly assess and identify external and internal anatomy.
Careful removal of the pulp chamber roof is carried out using a non-end cutting to avoid damage to the pulpal floor. Dark developmental lines on the floor of the pulp chamber should be observed like a ‘road map’ to identify possible root canals present.
Careful observation of the pulp chamber floor may also indicate additional root canal anatomy using sodium hypochlorite which may effervesce.
Use of the dental operating microscope or dental loupes with adequate illumination is essential to correctly identify internal anatomy and avoid iatrogenic damage to the floor of the pulp chamber.
Access cavity preparation does not need to be extended beyond the marginal ridge (see Fig. ). Loss of marginal ridge greatly reduces the strength of the tooth.
Clinical photographs demonstrating access cavity preparation and refinement during the treatment of a maxillary permanent first molar. Note () calcified floor of pulp chamber with only DB canal located, () ultrasonic troughing carried out, () DB and P canal orifices located, () MB1 canal orifice located, (e) MB2 canal orifice located and () final four canals cleaned and shaped. Access cavity is not extended beyond marginal ridge (red dash line)
Refinement of the access cavity will be required in the mesio-palatal direction using a rhomboid access. The MB2 canal is often palatal and often mesial in a line drawn between the MB1 and the palatal canal (see Fig. ).
Use of methylene blue dye stains can be useful to highlight the pulp chamber anatomy.
Trough and search with a low-speed bur or ultrasonic tip beginning from the MB1 orifice. Be careful not to exceed a depth of 2–3 mm.
Only gold members can continue reading. Log In or Register to continue
Tooth, Root, and Canal Anatomy
1.1 Introduction

Common methods for the study of root and canal morphology in extracted teeth. (a) Staining and clearing. (b) 2D radiographic imaging with different views. (c) Stereomicroscopy. (d) Scanning electron microscopy. (e) Cone beam computed tomography. (f) Micro-computed tomography.

Common methods for the study of the root and canal morphology in clinical practice. (a) 2D radiographic imaging. (b, c) Clinical identification using magnification, exploration, and troughing. (d) Identification using hand files. (e, f) Cone beam computed tomography in mandibular (e) and maxillary (f) teeth.
1.2 Different Perspectives in Characterizing Root and Canal Morphology
1.2.1 Deficiencies of Current Classification Systems for Root Canal Morphology

1.2.1.1 No Consideration of the Number of Roots in Anterior and Premolar Teeth

Application of the Vertucci classification in teeth with different root canal configuration types. Teeth with 2 separate root canals in (a) single-rooted, and (b) double-rooted maxillary premolars are classified as Type IV. Teeth with root canal configuration (1-2) in (c) single-rooted, and (d) double-rooted mandibular premolars are classified as Type V. Vertucci Type VIII can be presented in (e) double-rooted and (f) three-rooted maxillary premolars with three root canals.
1.2.1.2 Absence of Clear Definitions of Root Canal Components

In addition, there is confusion with regards to apical canal bifurcations – when it is a part of the configuration and when it is considered as an accessory canal. Similar confusion exists for apical root bifurcations whether a tooth with a bifid/small double root apex is considered as a single- or double-rooted tooth, which is discussed later in this chapter.
1.2.1.3 Non-classifiable Root Canal Configurations
1.2.2 Introduction to the New Coding System for Root and Canal Morphology
1.2.2.1 Terminology
- – Root canal system:
The space within the tooth that contains pulp tissue. The root canal system is divided into two portions: the pulp chamber and the root canals.
- – Pulp chamber:
The portion of the pulp space within (or extending to just below) the anatomic crown of the tooth. In single-rooted teeth and double/multi-rooted teeth with middle or apical root bifurcations with a single canal coronally, it extends to the most apical portion of the cervical margin of the crown, and in double/multi-rooted teeth with coronal root and/or canal bifurcations (no single canal coronally), it extends to the floor of the pulp chamber located in the coronal third of the root. A chamber (accessory) canal is a small canal leaving the pulp chamber that (usually) communicates with the external surface of the root (including the furcation). It can be of any type (patent, blind, or loop).
- – Root canal orifice:
The opening of the canal system at the base of the pulp chamber where the root canal begins. Generally, it is located at or just apical to the cervical line.
- – Root canal configuration:
The course of the root canal system that begins at the orifice and ends at the canal terminus (minor apical diameter).
- – Major apical foramen:
The exit of the root canal onto the external root surface, which is normally located within 3 mm of the root apex.
- – Minor apical foramen/apical constriction:
The apical part of the root canal with the narrowest diameter which is generally 0.5–1.5 mm from the major apical foramen. It is the reference point often used as the apical termination of canal instrumentation and filling procedures.
- – Accessory canal:
A small canal leaving the root canal that (usually) communicates with the external surface of the root or furcation. Hence, it can be located anywhere along the length of the root (coronal, middle, or apical third) and can be any type (patent, blind, loop) (Figure 1.6). It also includes what have been in the past termed lateral canals. Apical delta (or apical ramifications) is the region at or near the root apex where the main canal divides into multiple accessory canals (more than two).

Types of accessory canals – Patent, blind, loop and delta.
1.2.2.2 Classification
The new classification includes codes for three separate components: the tooth number, the number of roots, and the root canal configuration.
1.2.2.2.1 Tooth Number
The tooth number (TN) can be written using any numbering system (e.g. universal numbering system, Palmer notation numbering system, FDI World Dental Federation numbering system). If the tooth cannot be identified using one of the numbering systems (i.e. extracted teeth), then a suitable abbreviation can be used, for example UCI for upper (maxillary) central incisor (UCI).
1.2.2.2.2 Number of Roots
The number of roots (R) is added as a superscript before the tooth number (RTN). For instance, 1TN means that the tooth has one root. Any division of a root, whether in the coronal, middle, or apical third, will be coded as two or more roots. Accordingly, a bifurcation is represented as 2TN, and trifurcation is represented as 3TN and so on.
1.2.2.2.3 Root Canal Configuration

Application of the new coding system in single- rooted teeth.

Application of the new coding system in double-rooted teeth.

Application of the new coding system in three- rooted teeth.

Application of the new coding system to describe the common canal below the pulp chamber.
1.2.2.2.4 Location of Accessory Canals
The new coding system can also be used to classify accessory canals with canal configurations in a single code. The length of the root is divided into thirds (T): the coronal third (C), which starts from an imaginary line from the most apical portion of the pulp chamber, middle third (M), and apical third (A) ending at the canal terminus. Each third is identified as a superscript within parenthesis after the root canal configuration. In some instances, the accessory canal may not end in a foramen and in that situation, configuration code (1‐0) will describe a blind accessory, and code (2‐1‐0) will describe a looped accessory canal. Figures 1.11 and 1.12 show the application of the new coding system for accessory canals.

Application of the new coding system to describe different locations and types of accessory canals. (A1) refers to one accessory canal in the apical third. (M1) refers to one accessory canal in the middle third. (C1) refers to one accessory canal in the coronal third. (D) refers to apical delta. (M1, D) refers to the presence of one accessory canal in the middle third, and an apical delta.

1.2.2.2.5 Presence of Dental Anomalies
The new coding system can be adapted for root anomalies by including codes for anomalies and their subtypes (if present). The abbreviation of the anomaly (A) is added between brackets. For example,
- (DE) refers to dens evaginatus affecting a given tooth. If more than one of the same anomaly exists in one tooth, then the number is written on the left of the anomaly. Thus, (2A) describes a tooth with two of the same anomaly; thus, (2DE) describes a tooth with two dens evaginatus.
- When the tooth has two or more different developmental anomalies, a comma (,) should be added between the initial letters of each anomaly (A1, A2). Thus, (DI, RD) describes a tooth with both a dens invaginatus (DI) and a root dilaceration (RD).
- A slash (/) should be used in fused teeth, for example, fusion of one tooth to a supernumerary tooth, or fused roots in double-rooted teeth such as C-shaped canals occurring in fused double-rooted mandibular molars [44]. Two slashes (//) should be used in fused teeth or roots with intercommunications in the root canal and/or pulp chamber.
- The subtype of each classified anomaly (if present) should be written as a superscript after the abbreviation of the anomaly. Thus, (DII) describes a tooth with a dens invaginatus type I [45, 46]. In some instances, it may be impossible to define a subtype of the anomaly during an examination (such as during conventional radiographic examination), or when it is not relevant within a specific clinical or experimental report; in such cases, writing the abbreviation of the anomaly without a subtype would be sufficient.
Figures 1.13 and 1.14 show the application of the new coding system in teeth with dental anomalies.


Application of the new system to describe a mandibular molar with radix entomolaris. The observer can use the new system to describe only the root canal configuration or root canal configuration and accessory canals, or root canal configuration, accessory canals and anomalies.
1.2.2.3 Applications of the New System in Teaching

1.2.2.4 Applications of the New System in Research

1.2.2.5 Applications of the New System in Clinical Practice
The interpretation of root canal morphology could vary through the phases. An example, based on the 2D pre-operative radiographic image in Figure 1.17, the operator would categorise this as a double-rooted tooth 36 in which the mesial root (M) appears to have two separate canals and the distal root (D) appears to have one canal configuration. Therefore, the initial code for this tooth is 236 M2 D1 (Figure 1.17a). After root canal instrumentation and filling, two accessory canals were noted in the apical thirds of each of the mesial and distal root (Figure 1.17b). Therefore, the code was eventually 236 M2(A1) D1(A1), which refers to double-rooted tooth 36 in which the mesial root has 2 separate canals and a single accessory canal in the apical third of the root, while the distal root has one canal and a single accessory canal in the apical third of the root. Another example is shown in Figure 1.17c,d. This means that the new coding system can be modified based on the operator’s interpretation along the treatment phases from diagnosis to root canal filling – or during surgery.

The interpretation of root canal morphology using the new coding system during the observational phase is important, especially for undergraduate and postgraduate students as well as GDPs where cases have to be pre-evaluated carefully to fit their level of knowledge and experience. This means a tooth code 234 B1-2 L1 (double-rooted tooth 34 in which the buccal root is assumed to have canal configuration 1-2 and the lingual root has one canal) interpreted from a 2D pre-operative radiograph may not be suitable for an undergraduate dental student, and a tooth code (RD) 236 M2 D2 (double-rooted tooth 36 in which both mesial and distal roots are dilacerated – RD – Root Dilaceration) may not be suitable for a GDP. Therefore, the new system can play a role in assessing case difficulty at the pre-operative stage, and also can provide a single code of the tooth after treatment, which may show other anatomical features, such as accessory canals.
1.2.2.6 Limitations and Technical Challenges
The interpretation of canal anatomy using the new coding system (as well as other classification systems) is highly dependent on the method used (i.e. staining and clearing, 2D radiographic, CBCT or micro-CT). Indeed, micro-CT is able to show the fine details including delicate canal branching and accessory canals, which cannot be seen in CBCT images; therefore, the coding of the same tooth using both techniques will be different.
1.3 Advances in Apical Canal Morphology
The anatomical landmarks of the apical root canal have been investigated since the beginning of the twentieth century. The development of new imaging systems has generated substantial data to increase knowledge regarding the morphological characteristics of the apical region of the root and root canal, such as the cemento-dentinal junction (CDJ), apical constriction (AC), apical foramen (AF), isthmuses, accessory canals (ACCs), and bifid root apices (Figure 1.18).

Examples of the morphological characteristics of the apical region of roots and root canals.
1.3.1 Cemento-dentinal Junction (CDJ)
1.3.2 Apical Constriction (AC)

The apical constriction, just coronal to the apical foramen, is defined as the smallest diameter of the root canal.

In longitudinal sectioning, the section must be at the centre of the canal throughout its path to allow accurate measurements. The topography and the location of the AC varies amongst the longitudinal sections even though the interval between the sections is in microns. Also, the smallest diameters of root canal in different directions are at the same level of the root only in completely round root canals. As root canals are not completely round in the apical third, the smallest diameter displayed in longitudinal sections in different directions may not be at the same level of the root.

The white lines show the proper position and direction of the plane of longitudinal section to accurately measure the smallest diameter of canal at different levels of three roots. Yellow-black hatched areas show the area of the canal.
1.3.3 Major Apical Foramen (MAF)

Micro-CT view of the deviation of the apical foramina. Blue arrow shows the apical foramen of middle mesial canal (MM), which terminates 7 mm from the root apex.
In recent years, the number of studies examining the entire apical root canal has increased. In these studies, 2D measurements such as area, perimeter, minor and major diameters, form factor, and roundness of the apical root canal have been measured at 0.5 mm or 1 mm intervals. In addition, surface area, structure model index (SMI) and volume of the canal have been measured independent of the operator’s experience as 3D measurements (Table 1.1) (Figure 1.23). These detailed and precise 2D and 3D measurements from the apical root canal third are expected to guide clinical procedures.

2D measurements (area, perimeter, major and minor diameters form factor and roundness) of apical root canal of mandibular incisor in 0.5 mm intervals from the AF. Also, 3D measurements (volume, surface area, and SMI) of entire root canal space.
2D and 3D morphometric parameters used to examine root canal geometry.
1.3.4 Isthmus

Micro-CT view of the isthmus roof and isthmus floor.



Two-dimensional axial images of the same sample show debris accumulation within the isthmus.
1.3.5 Accessory Canals and Apical Deltas
Only gold members can continue reading. Log In or Register to continue
Choosing the GentleWave® Procedure
If you’ve been diagnosed with a root canal system infection and are seeking a root canal alternative that can help save your natural tooth4, the GentleWave Procedure is what you’ve been looking for.
To find a nearby GentleWave Doctor, use our Doctor Locator today!
Ready to Discover the Beneficial GentleWave Procedure?
The GentleWave Procedure is an innovative root canal treatment option that offers patients the chance for fewer appointments,4 fast healing4 and the opportunity to save their natural tooth. Ready to experience this state-of-the-art treatment option? Schedule a consultation today by finding a nearby GentleWave Provider using our Provider Locator!
The GentleWave® Procedure is a medical procedure that is designed to prepare, clean and preserve the structure of teeth1,2,4 indicated for root canal therapy. Similar to other root canal treatment procedures, there is a potential risk of adverse effects. If you are considering the GentleWave Procedure, ask your clinician if you are a proper candidate. For additional information, visit https://gentlewave.com/safety-information.
8 Things You Should Know About Root Canals
Are you concerned that you may have a root canal system infection? Or has your dentist or endodontist told you that you need a root canal? With the many misconceptions around root canal therapy, you might hear “root canal” and start to experience panic or anxiety.
To help ease any worries, we’ve compiled a list of some important information you should know about root canals to help you better understand what a root canal system infection is and how you can best address the issue.
Read on to have your questions about root canals answered—and learn some things you might not know about root canals!
1. What is a Root Canal?
A “root canal” is the term used to describe the cavity within the center of the tooth*, but it’s also commonly used to describe the treatment of an infected root canal system. Your tooth’s nerves and pulp live within the root canal and if they become infected, it’s important to schedule an appointment with your dental provider immediately to avoid further issues, like an abscess.*
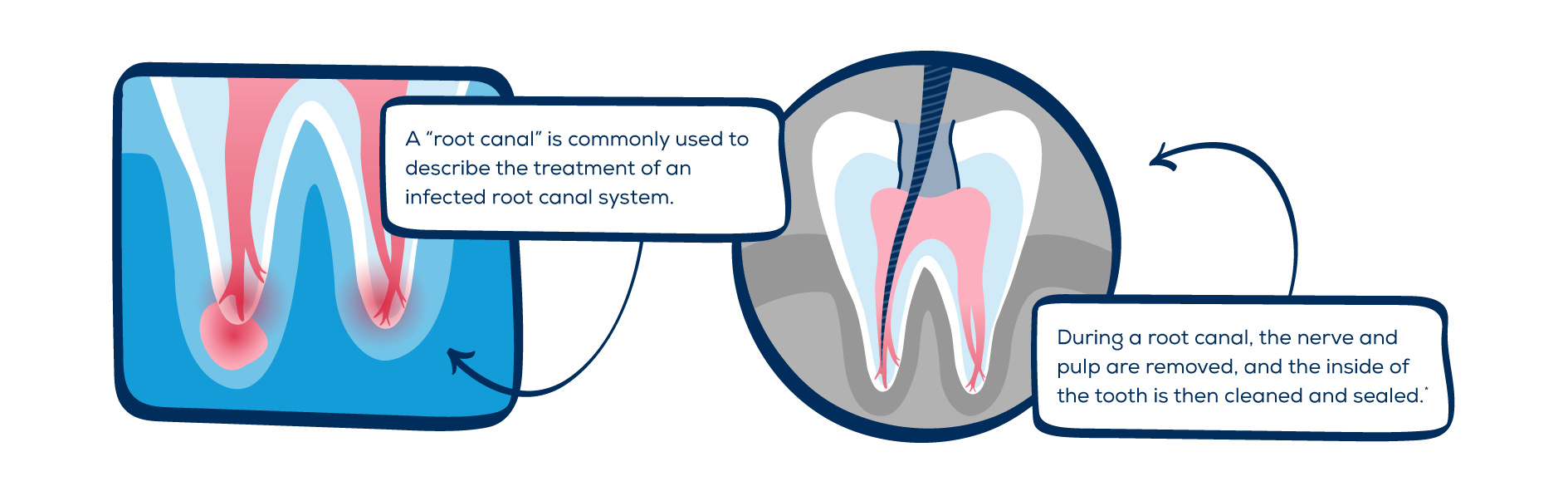
During a root canal, the nerve and pulp are removed, and the inside of the tooth is then cleaned and sealed.* It’s important to note that a root canal does not kill the tooth. While root canals do remove the nerves inside the tooth, these nerves serve little function in a fully formed tooth. Once your root canal is complete, your tooth will continue to function normally.**
2. What’s the History of Root Canals?
The history of endodontics started in the 17th century when the first techniques of dental transplants were documented.*** In fact, the first root canal instrument was constructed from a watch spring in 1838*** and was used to access the pulp within the root of the tooth.
Advancements in root canals continued, which led to the introduction of the filling material, gutta-percha, in 1847.*** Gutta-percha is often used after the tooth is cleaned and disinfected to help fill and seal it†, and it continues to be used today for this purpose during most root canals.
Fortunately, thanks to the efforts of many researchers and specialists, root canals have come a long way—and patients can be confident that they are a reliable and safe endodontic therapy.***
3. What Are the Primary Symptoms of a Root Canal?
There are various root canal symptoms to be aware of, and understanding what to look for is key in ensuring you receive timely treatment.
Common root canal symptoms include:
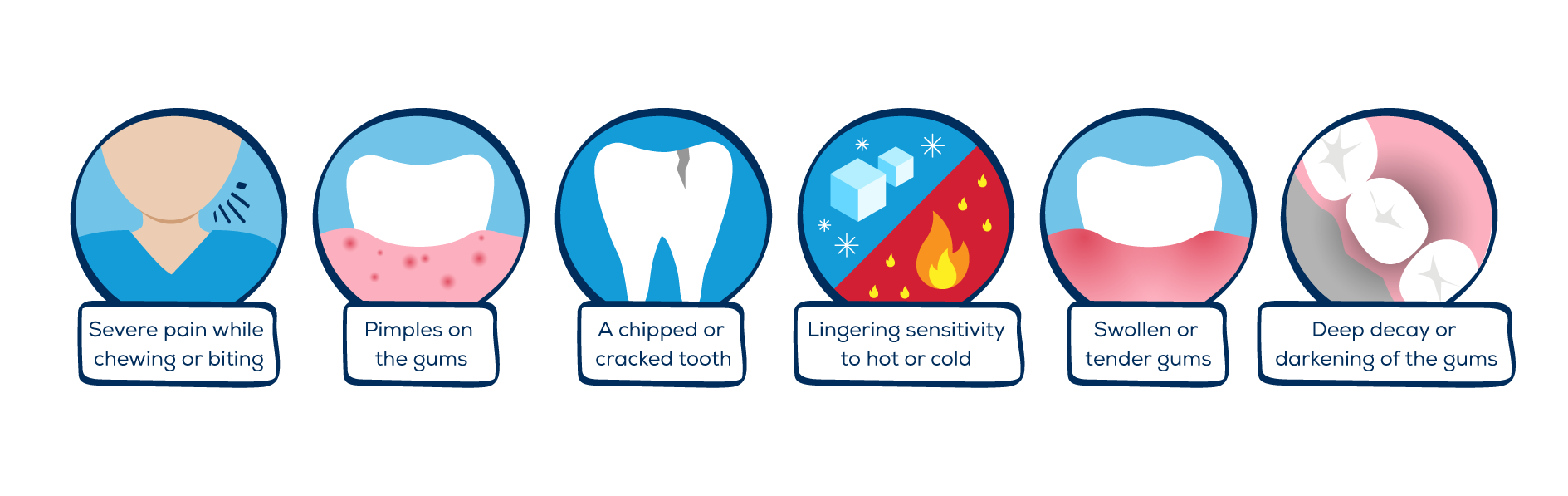
- Severe pain while chewing or biting;
- Pimples on the gums;
- A chipped or cracked tooth;
- Lingering sensitivity to hot or cold, even after the sensation has been removed;
- Swollen or tender gums, and;
- Deep decay or darkening of the gums†
If you find that you are experiencing one or more of these root canal symptoms, be sure to schedule an appointment with your dentist or endodontist immediately.
4. Should I Choose a Dentist or Endodontist?
An endodontist is a dentist who has additional schooling and specialization in the causes, diagnosis, prevention and treatment of diseases and injuries of the dental pulp or nerve of the tooth.* These individuals are considered to be root canal specialists who can handle all root canals—but especially more complex cases.
Be sure to discuss with your dentist who is the best candidate for handling your root canal and if they prefer you work with an endodontist, request a referral to one they would recommend.
5. What Are My Root Canal Options?
The most well-known root canal option is standard root canal treatment. During standard root canal treatment, files and treatment fluids are used to remove the infected pulp tissue, and the interior of the tooth is cleaned, filled and sealed.
Patients suffering from a root canal system infection may also choose to remove the infected tooth and replace it with a dental implant. This process includes the insertion of a metal post in the jaw with an affixed porcelain crowns—and typically these procedures cost more than an endodontic treatment.†
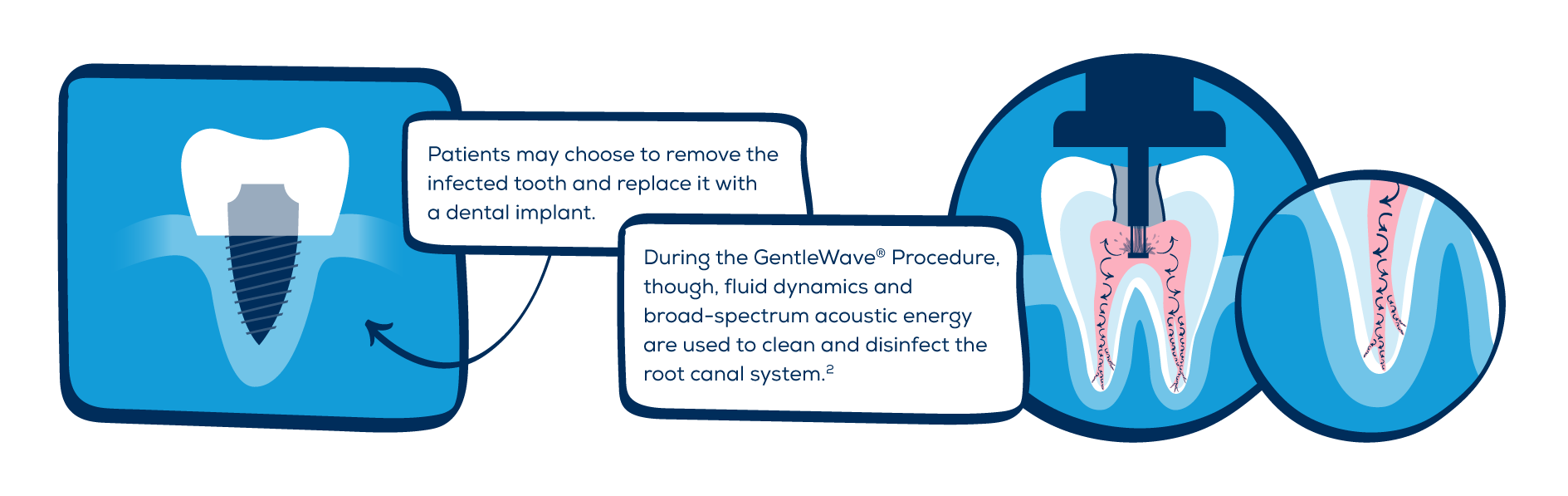
During the GentleWave® Procedure, though, fluid dynamics and broad-spectrum acoustic energy are used to clean and disinfect the root canal system. 2 This alternative root canal option is so effective at cleaning the root canal system,1,2 there’s less chance of failure over time,4 helping patients save their natural tooth.4
6. What Are the Advantages of Saving My Natural Tooth?
Saving your natural tooth offers a number of advantages, including:
- Efficient chewing;
- Normal biting force and sensation;
- Natural appearance, and;
- Protecting other teeth from excessive wear or strain†
Make sure to discuss with your dentist or endodontist which treatment option will help you save your natural tooth so you can experience the long-term benefits of preserving your smile.
7. Will I Feel Pain During My Root Canal?
Many endodontic procedures are performed to actually relieve the pain of toothaches caused by inflammation or infection. With modern techniques, root canals are relatively painless.† In fact, a lot of patients report that they are comfortable during the procedure, and it can typically be completed in just one to two appointments.††
While you may experience some sensitivity or discomfort the first few days after a root canal, this can typically be relieved with over-the-counter medications. You’ll be back to biting, chewing—and smiling—with ease in no time.†
8. What Should I Expect from My Root Canal Recovery?
Proper care of your treated tooth is a must for a successful root canal recovery. You should avoid eating for a few hours until the numbness in your mouth wears off† to help avoid biting your cheek or tongue. After that, it’s important to stick to soft foods that require little chewing to help minimize the risk of hurting your teeth.
In all, with proper care and attention, your treated tooth can stay healthy forever.††
Ask the Endodontist
Question: What are the differences between a dentist and endodontist?
Answer: All endodontists are general dentists first, but an endodontist receives 2-3 years of further training in endodontics, which is treatment of the dental pulp and surrounding tissues. The biggest difference beyond the additional education is that an endodontist is a root canal specialist who will treat root canals all day, every day. Depending on the practice, a general dentist may only perform one to two root canals per week—but an endodontist will typically perform up to ten root canals every day.
Question: Are there advantages or disadvantages to choosing an endodontist over a dentist for a root canal procedure?
Answer: Seeing an endodontist can lead to more efficient treatments, and these root canal specialists also have multiple technologies that a general dentist might not. These include a range of advanced options like the GentleWave® Technology, which is the most effective and efficient way to clean root canals. This translates to higher success rates, faster healing and less post-operative sensitivity.
Question: Which of the root canal treatment options—dental implants, standard root canal treatment or the GentleWave® Procedure—would you consider more beneficial for patients in terms of long-term results?
Answer: In most cases, root canal therapy is the best option and offers the most benefits to the tooth. It allows for complete cleansing of the canals and restoring the tooth back to normal bite function. Even root canal retreatment is usually more desirable than a surgical approach, as it allows patients to retain all of their root structure.
In general, the GentleWave Procedure cleans the canals so well, it offers a better chance for success. I now even approach advanced infections very differently. Before the GentleWave Procedure, I would often recommend extraction if a tooth appeared to have an infection indicative of a root fracture. Now, though, I am more inclined to at least open a tooth and see what we find. If there is a fracture, then the tooth still has to be removed—but, if there is no evidence of fracture, we are now completing these cases in a single visit of about an hour and are noticing incredible healing.
Question: How does the process for standard root canal treatment differ from the GentleWave Procedure?
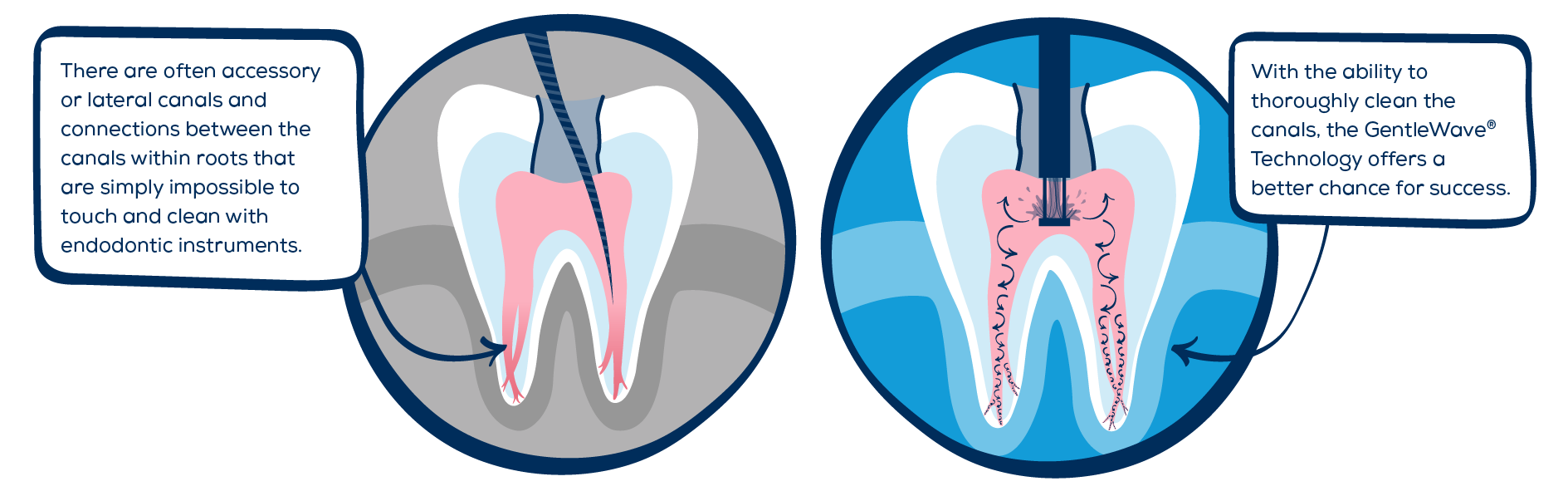
Answer: Historically, the problems with root canals have stemmed from having to clean the intricate anatomy, which is formed by blood vessels. There are often accessory or lateral canals and connections between the canals within roots that are simply impossible to touch and clean with endodontic instruments. This meant that the standard root canal process involved opening the canals wide enough to allow for disinfectants to reach the root tips, where most of the anatomy can be complex.
For me, it also meant multiple visits to allow enough time to hopefully remove all of the tissue and debris from the canals. In the most advanced infections, this sometimes meant working on a tooth three or four times over a period of up to six months. While I was able to achieve success with this, it wasn’t convenient for anyone involved, especially the patient who had to sit through multiple visits until we were confident of eventual healing and success.
With the GentleWave Procedure, though, the root canal process has changed. We can now keep the canals very small, and we only do conservative canal preparations, which retains precious dentin in the roots. This gives more structural stability for the tooth. Additionally, standard root canal procedures predispose teeth to root fracture more often, which can lead to tooth loss. The GentleWave Procedure is a much better approach in my opinion.
“I have seen remarkable and almost miraculous healing of even really advanced infections when performing the GentleWave Procedure.”
Question: How long does standard root canal treatment take compared to the GentleWave Procedure?
Answer: Standard root canal treatment takes significantly more time than the GentleWave Procedure. With standard root canal treatment, the canals must be shaped to an adequate size to allow disinfectants to reach the tooth apices, then the disinfectant needs to sit in the tooth for a minimum of 40-60 minutes before sealing the roots and completing the treatment. For me, this was often achieved over multiple visits to allow sufficient time between appointments with the medicaments in the canals to better disinfect the roots.
“The healing happens much faster than what I’ve seen in my 10 years of practice prior to incorporating the GentleWave Procedure, and patients are experiencing less post-operative pain.”
Question: What are the common symptoms after a root canal procedure that patients can expect? What level of pain after root canal treatment is normal, and how does it compare between treatment options?
In general, though, the post-operative pain levels after the GentleWave Procedure are less than standard root canal treatment. Most patients experience very little or no pain, and the tooth feels better almost immediately. There are still cases that take more time to settle back to normal, but they are far fewer than treatment without the GentleWave Procedure.
Question: How can patients ensure long-term success of their tooth after treatment?
If a crown is required, it is best to contact your dentist within 24 hours to schedule that. The crown may be done at any time, ideally within the first 30 days. Beyond that time, the filling may leak, which could lead to re-infection of your tooth.
Question: What is the biggest benefit of the GentleWave Procedure for your patients?
Answer: The biggest benefit of the GentleWave Procedure is that we are saving more teeth in less time with less removal of healthy dentin. This means that patients are back to themselves sooner and can move on with life without the nuisance of a toothache.
“I believe we will see better long-term success with the GentleWave Procedure.”
An Alternative to Standard Endodontic Treatment
The GentleWave Procedure is an alternative to standard endodontic treatment that uses fluid dynamics and broad spectrum acoustic energy to clean and disinfect the root canal system.2 Since this procedure does not primarily rely on the use of files, it’s able to reach and disinfect the microscopic twists and turns of the root canal anatomy.2,3
Keep scrolling down to see just how simple it is for the GentleWave Procedure to clean and disinfect such complex anatomies!

Are you looking for an alternative to standard root canal treatment? Find a GentleWave provider in your area.
The GentleWave® Procedure is a medical procedure that is designed to prepare, clean and preserve the structure of teeth1,2,4 indicated for root canal therapy. Similar to other root canal treatment procedures, there is a potential risk of adverse effects. If you are considering the GentleWave Procedure, ask your clinician if you are a proper candidate. For additional information, visit https://gentlewave.com/safety-information.
Standard Endodontic Treatment
But, as you see in the infographic below, root canal systems are complex. It can be difficult for files and treatment fluids alone to successfully remove all of the infected tissue and bacteria—not to mention the fact that bacteria likes to hide within the microscopic “nooks and crannies” of the canal wall!
That’s where the GentleWave® Procedure comes in!
What is Endodontics?
Endodontics is the area of dentistry that specializes in the treatment of the tooth’s interior, or the dental pulp—the tissue within the root canal system of a tooth.
")




")